Tim Alexander Ubenauf, Germany
Department of Pediatric Kidney, Liver and Metabolic Diseases
Medizinische Hochschule Hannover
Native T1-time in cardiac MRI suggesting myocardial fibrosis is elevated in young kidney transplant recipients
Jeannine von der Born1, Tim Ubenauf1, Carl Grabitz1, Nima Memaran1, Rizky Indrameikha Sugianto1, Nele Kanzelmeyer1, Bernhard MW Schmidt2, Jan Falk3, Diane Renz3, Anette Melk1.
1Clinic of Pediatric Kidney, Liver and Metaboilic Diseases , Hannover Medical School , Hannover , Germany; 2Clinic for kidney and hypertension diseases, Hannover Medical School , Hannover , Germany; 3Institute for Diagnostic and Interventional Radiology , Hannover Medical School , Hannover , Germany
Background: Cardiovascular morbidity after kidney transplantation (KTx) during childhood is common and leads to increased mortality. In adults with chronic kidney disease (CKD) myocardial fibrosis impairs cardiac relaxation and causes diastolic dysfunction. Native T1 relaxation time (nT1) in cardiac MRI resembles diffuse myocardial fibrosis. As there is no data on myocardial fibrosis in patients after pediatric KTx, we aimed to comprehensively assess left ventricular (LV) systolic and diastolic function with special focus on septal nT1 in cardiac MRI.
Methods: 46 KTx patients (mean age 16 ± 3.5 years; 7.9 ± 5.3 years after KTx) and 46 sex- and age- matched healthy controls were examined with gadolinium-free cardiac MRI and echorcardiography. nT1 (a surrogate marker for myocardial fibrosis) was measured at the interventricular septum at a basal and mid-ventricular short-axis slice. Parameters derived from echocardiographic examinations included left ventricular mass index (LVMI) and measures of LV diastolic function (E/A-ratio, E/e´, isovolumetric relaxation time (IVRT), left atrial dimensions, pulmonary venous flow). T test was used to compare KTx patients and controls. Multivariable linear regression analysis was used to evaluate the association between echocardiographic parameters and nT1 as well as clinical parameters associated with nT1.
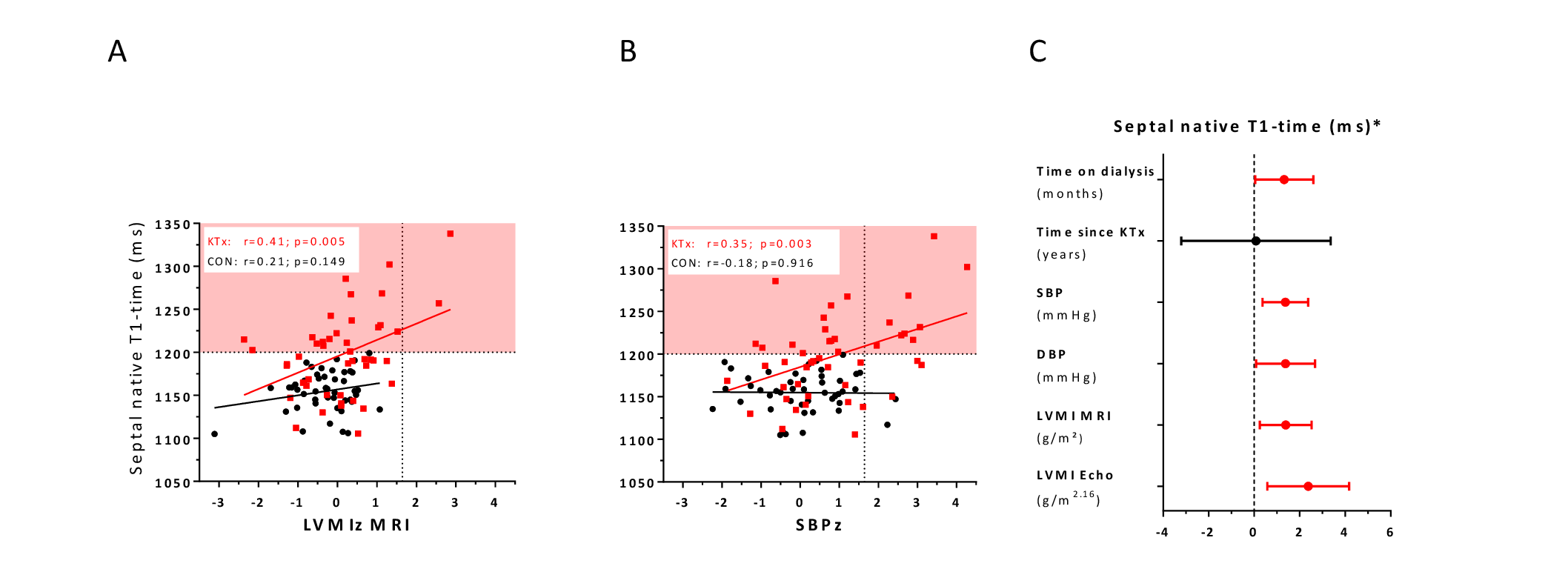
Results: Young KTx recipients had a siginficant higher nT1 at the interventricular septum than healthy controls (1198 ± 48.8 ms vs. 1155 ± 23.4 ms; p< 0.001). In KTx recipients, LVMI z-score (LVMIz) was higher (0.1 ± 1.1 g/m2 vs. -0.3 ± 0.7 g/m2; p=0.026) and GLS was lower than in healthy controls (-19 ± 2.1 % vs. -20.3 ± 2.7%; p=0.010). LVMIz (derived from MRI and Echo) and systolic (SBP) and diastolic blood pressure (DBP) were associated with higher nT1 in patients, but not in controls (Fig. 1A/B). Time on dialysis was significantly associated with nT1, whereas time after KTx was not .
Conclusion: A significant higher nT1 in young KTx recipients suggests early myocardial fibrosis. Classical echocardiographic parameters do not sufficiently reflect these early changes. Cardiac MRI may be an important tool in detecting early cardiovascular damage in children after KTx.
Lectures by Tim Alexander Ubenauf
| When | Session | Talk Title | Room |
|---|---|---|---|
|
Tue-28 08:00 - 09:00 |
Kidney 4 | Native T1-time in cardiac MRI suggesting myocardial fibrosis is elevated in young kidney transplant recipients | Zilker 3-4 |