Physiotherapist
Rehabilitation
Hospital for Sick Children, Department of Rehabilitation Services
Functional performance and fitness in pediatric lung transplant candidates and recipients: a retrospective review
Robin Deliva1,2,4, Hartmut Grasemann2,3,4, Melinda Solomon2,3,4.
1Physiotherapy, Hospital for Sick Children, Toronto, ON, Canada; 2Transplant and Regenerative Medicine Centre, Hospital for Sick Children, Toronto, ON, Canada; 3Respirology, Hospital for Sick Children, Toronto, ON, Canada; 4University of Toronto, Toronto, ON, Canada
Background: Exercise performance is reduced in children with end-stage lung disease and after lung transplant (LTx). Limited studies have examined fitness from a functional perspective. We examined muscle strength, endurance, motor proficiency and self-reported fatigue and sought to identify factors associated with outcomes.
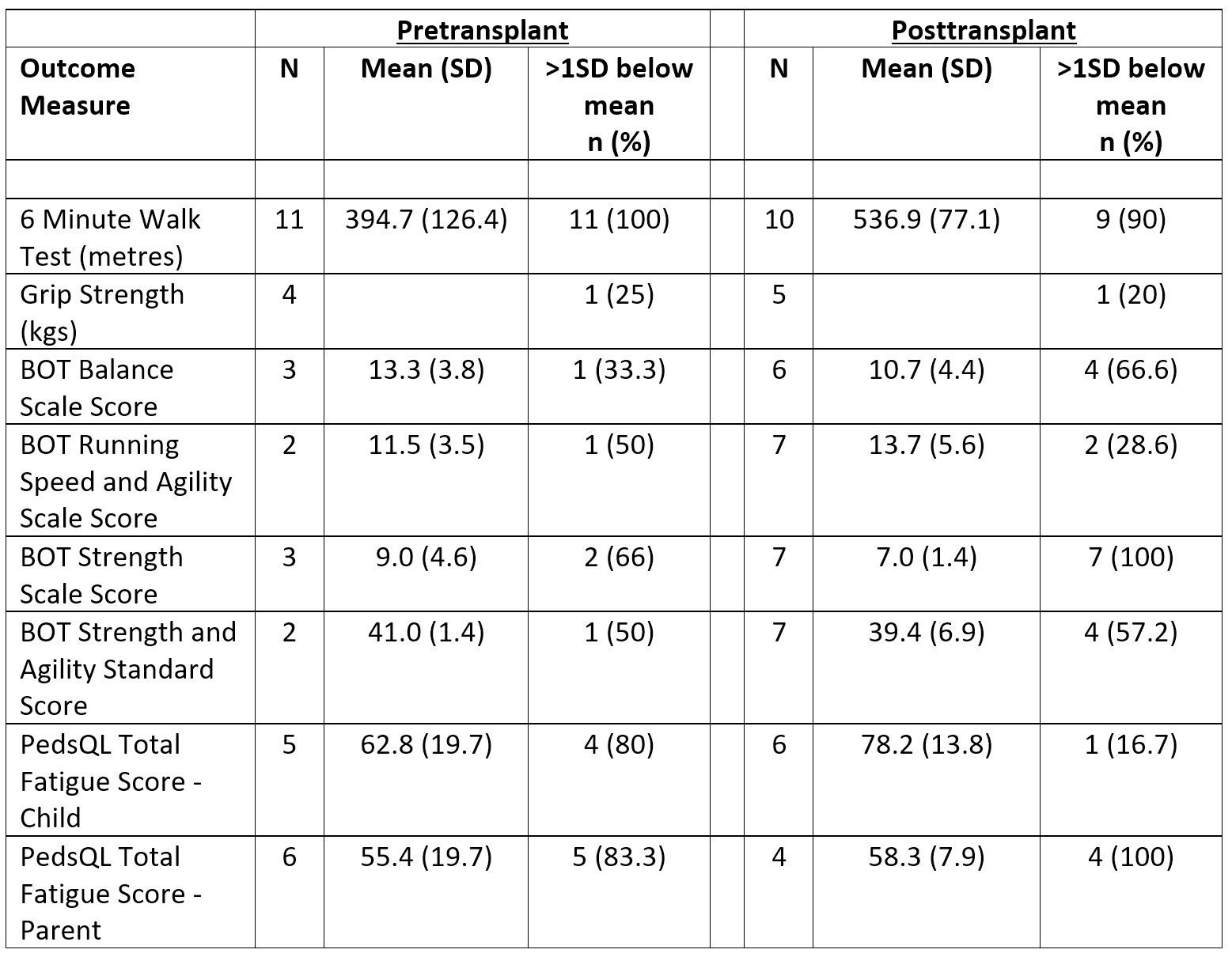
Methods: Single centre, retrospective review of pre- and one-year post-LTx assessments (Ax) in children who were listed and/or underwent LTx at ≥6 years of age between Jan 1, 2013 - Apr 1, 2019. Standardized Ax included: Six-minute walk test (6MWT), components of the Bruininks-Oseretsky Test of Motor Proficiency 2nd Ed (BOT) and Pediatric Quality of Life (PedsQL) fatigue module (child and parent-proxy). Results were compared to published age and sex-matched norms: below average defined as >1 standard deviation (SD) below mean.
Results: Sixteen children met criteria [11 (69%) female; age at LTx 13.3±3.3y]; underwent LTx [cystic fibrosis (7; 44%), pulmonary hypertension (4; 25%), bronchiolitis obliterans (3; 19%), other (2;12%)] with pre-LTx ECMO/Novalung support in 4 (25%). Two (12%) had previous neurological diagnosis and 2 (12%) suffered neurological injury perioperatively. Status at listing was high priority for 7 (44%) and 4 (25%) required inpatient rehabilitation post-LTx. Results of initial pre- and post-LTx outcome measures are reported in Table 1. Pre-LTx mean BOT strength scores were below average and all children fell >1SD below mean on 6MWT. Eight children (50%) underwent physiotherapy in the pre-LTx period with a 3-month improvement in 6MWT (402.5±136 to 508.2±78 metres; p=0.077). High levels of fatigue were reported by children and parents. Post-LTx, BOT strength scores were below average and significantly below population mean (p<0.001). 9/10 (90%) scored >1SD below the mean on the 6MWT. A post-LTx 6MWT distance >2 SD below mean was associated with a higher listing status (p=0.008). Seven children completed a 6MWT both pre- and post-LTx assessment with a significant improvement in distance (400.6 ± 155.2 to 555.7 ± 78.0 metres; p=0.005). Challenges to performing standardized physical assessments pre-LTx included medical acuity, activity intolerance and technological constraints. Post-LTx challenges included patient relocation and transitioning to adult care.
Conclusion: Functional outcome measures suggest significant limitations in physical fitness in pediatric LTx candidates and recipients. Muscular strength and 6MWT continue to be reduced one-year post-LTx. Pre-LTx physiotherapy programs may improve exercise tolerance in the waiting period, emphasizing the need for rehabilitation with a focus on strength and endurance training to optimize fitness prior to and recovery from LTx to improve long-term health.
References:
[1] Panepinto J et al. PedsQL Multidimensional Fatigue Scale in Sickle Cell Disease: Feasibility, Reliability and Validity. Pediatric Blood Cancer 2014; 61: 171-177.
[2] Geiger R. et al. Six-Minute Walk Test in Children and Adolescents. Journal of Pediatrics. 2007; 150: 395-9.
[3] Bohannan, R.W. et al Handgrip Strength: A Population-Based Study of Norms and Age trajectories for 3-17 year-olds. Pediatric Physical Therapy 2017; 29(2): 118-23
Lectures by Robin Deliva
| When | Session | Talk Title | Room |
|---|---|---|---|
|
Sat-25 17:00 - 18:00 |
Thoracic (Heart) | Functional performance and fitness in pediatric lung transplant candidates and recipients: a retrospective review | Hill Country CD |