Postdoctoral Researcher
Department of Pediatric Kidney, Liver and Metabolic Diseases
Hannover Medical School
Intensified systolic blood pressure control may regress left ventricular hypertrophy in children after kidney transplantation: a longitudinal analysis of 4C-T study
Rizky I. Sugianto1, Carl Grabitz1, Nima Memaran1, Karolis Azukaitis2, Anke Doyon3, Daniela Thurn-Valsassina1,4, Franz Schaefer3, Bernhard M. W. Schmidt5, Anette Melk1.
1Department of Pediatric Kidney, Liver and Metabolic Diseases, Hannover Medical School, Hannover, Germany; 2Clinic of Pediatrics, Faculty of Medicine, Vilnius University, Vilnius, Lithuania; 3Center for Pediatrics and Adolescent Medicine, University Hospital Heidelberg, Heidelberg, Germany; 4Department of Pediatrics and Adolescent Medicine, Medical University of Vienna, Vienna, Austria; 5Department of Nephrology, Hannover Medical School, Hannover, Germany
The 4C study.
Introduction: Left ventricular hypertrophy (LVH) affects about 40% of children one year after kidney transplantation (KTx) and strongly predicts cardiovascular mortality. Early after KTx, blood pressure (BP) is the main determinant of LV mass. Specific recommendations on BP goals in pediatric KTx recipients based on prospective data are currently not available. We aimed to assess the effect of BP control expressed by the cumulative exposure of systolic BP on the dynamics of left ventricular mass index (LVMI).
Methods: We included 96 children (64 males) ≥9 months post-KTx from the 4C study. BP and echocardiographic LVMI assessments were performed every 6 and 12 months, respectively. Only patients with two visits or more were included (median/maximum follow-up time of 2.5/7 years). The cumulative exposure of systolic BP z-scores was calculated for each visit as time-averaged area under the curve of BP z-scores (cAUC-SBP). cAUC-SBP was categorized into “<50th percentile”, “50th-75th percentile”, “75th-90th percentile”, and “>90th percentile”. Linear mixed regression model for LVMI (g/m2.16) for cAUC-SBP adjusted for time since baseline, age, sex, estimated glomerular filtration rate (eGFR), body mass index (BMI) z-score, LVMI at baseline was performed.
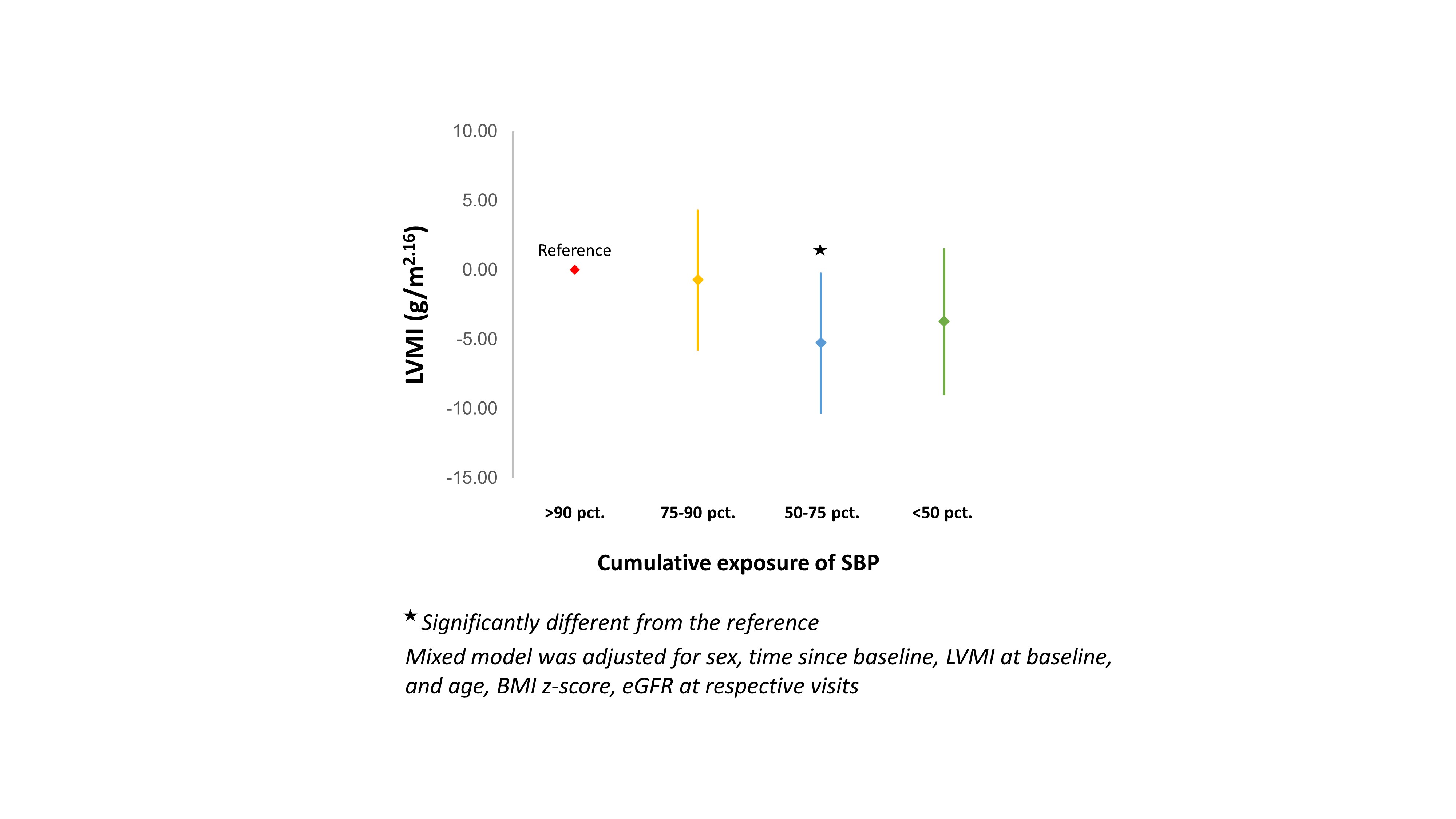
Results: At baseline, LVMI was 49.7±12.7 g/m2.16 and 64% (n=61) of patients showed LVH. Compared to patients with cAUC-SBP of >90th percentile, those with cAUC-SBP of 50th-75th showed LVMI reduction of -5.24 g/m2.16 (p=0.007) and those with <50th showed a tendency of reduction (β=-3.70 g/m2.16;p=0.067). Patients with cAUC-SBP of 75th-90th did not show a significant reduction (Fig. 1).
Conclusion: Continuous exposure to systolic BP values below the 75th percentile lead to regression of LVH. Our data calls for stricter BP control in pediatric KTx recipients.
German Federal Ministry of Education and Research (#01EO0802). European Renal Association – European Dialysis and Transplant Association (www.era-edta.org). Roche Organ Transplant Research Foundation (ROTRF, #365520785). One Lambda Inc. Fellowship Award of Women in Transplantation.
Lectures by Rizky I. Sugianto
| When | Session | Talk Title | Room |
|---|---|---|---|
|
Tue-28 08:00 - 09:00 |
Kidney 4 | Intensified systolic blood pressure control may regress left ventricular hypertrophy in children after kidney transplantation: a longitudinal analysis of 4C-T study | Zilker 3-4 |