
Amplified inferior outcomes for infant pediatric liver transplant candidates and recipients at low volume centers
Daniel Stoltz1, Kliment Bozhilov1, Amy Gallo1, Varia Kirchner1, Grant Lum1, Julianne Mendoza2, Carlos Esquivel1, Andrew Bonham1.
1Division of Transplant Surgery, Lucile Packard Children's Hospital Stanford, Palo Alto, CA, United States; 2Pediatric Anesthesia, Lucile Packard Children's Hospital Stanford, Palo Alto, CA, United States
Introduction: Low-weight pediatric liver transplant recipients have been shown to have inferior outcomes.1 This study aimed to compare patient and graft survival of low-weight pediatric liver transplant recipients at high volume (HV) and low volume (LV) transplant centers in the United States. It also aimed to identify discrepancies in waitlist mortality based on recipient weight at HV and LV centers.
Methods: Using the SRTR database, pediatric liver transplant recipients from 2010 through 2020 were identified. Transplant centers were designated as HV or LV based on the average number of pediatric liver transplants performed per year (HV: ≥ 5, LV: <5). Overall patient and graft survival up to 3 years post-transplant was calculated according to transplant center volume and recipient weight (<10kg and >10kg) and compared using Kaplan-Meier curves and log-rank tests. Waitlist mortality was calculated and compared between these groups.
Results: 4332 patients received transplants at HV centers (2635 patients >10kg, 1697 patients <10kg) and 876 patients received transplants at LV centers (624 patients >10kg, 252 patients <10kg). Patient and graft survival for recipients <10kg was worse at LV centers compared to HV centers (p<0.001 and p<0.001, respectively). Waitlist mortality was significantly higher at LV centers compared to HV centers for recipients <10kg (28.95 vs 16.5 events per 100 person-years; p<0.001).
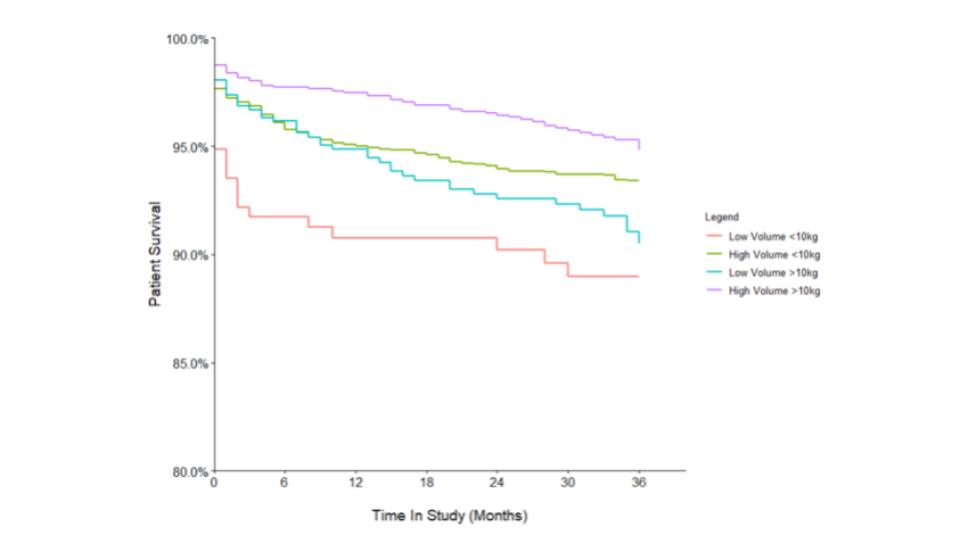
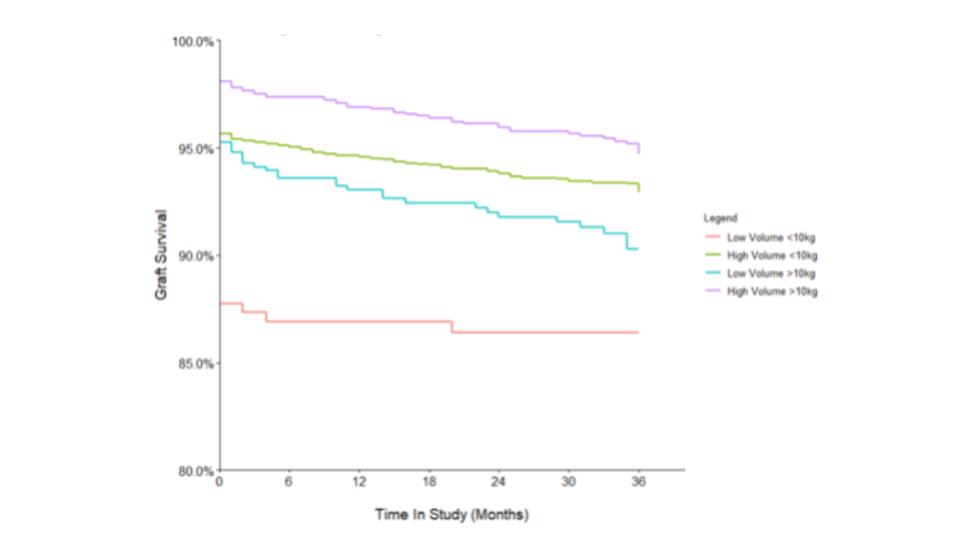
Conclusion: Low-weight pediatric liver transplant recipients have inferior outcomes at LV centers. Waitlist mortality for low-weight pediatric liver candidates is increased at LV centers. There is a need for collaboration between HV and LV centers to reduce waitlist mortality and improve transplant outcomes in this vulnerable population.
[1] Jain AK, Anand R, Lerret S, Yanni G, Chen JY, Mohammad S, Doyle M, Telega G, Horslen S. Outcomes following liver transplantation in young infants: Data from the SPLIT registry. Am J Transplant. 2021 Mar;21(3):1113-1127. doi: 10.1111/ajt.16236. Epub 2020 Sep 5. PMID: 32767649; PMCID: PMC7867666.
