
Treatment of refractory acute rejection with local graft irradiation in pediatric kidney transplant patients: A case series
Corinne M. Hite1, Katherine VandenHeuvel3, Charles D. Varnell2, Steve S. Woodle4, David K. Hooper2.
1Department of Pediatrics, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; 2Department of Nephrology , Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; 3Department of Pathology, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; 4Department of Transplant Surgery, University of Cincinnati Medical Center, Cincinnati, OH, United States
Introduction: Intravenous corticosteroids and anti-thymocyte globulin (ATG) are mainstays of treatment in patients with acute T-cell Mediated Rejection (TCMR). However, a subset of patients experience dose limiting side effects such as serum sickness or TCMR refractory to these therapies. Management of refractory TCMR is not well studied, especially in the pediatric population. Prior to widespread use of ATG, local graft irradiation (LGI) was used for treatment of refractory acute rejection in adults(1-7), but studies were poorly done and lacked biopsy assessment. In our center, we have used LGI in 3 patients with refractory rejection and report our results.
Case Presentation: We report 3 pediatric patients with cases of biopsy proven TCMR that were refractory to steroids and ATG on repeat biopsy since 2015. In 2 of the 3 cases, use of ATG was limited by development or history of serum-sickness reaction. All three patients were treated with LGI (1.5 Gy X 3 treatments) after either steroids or steroids & ATG, depending on above limitations in use of ATG. In 2 of 3 cases, the rejection resolved completely on follow up biopsy. In the remaining case, Banff grade 1A TCMR persisted after LGI but the patient was ultimately able to achieve complete resolution on biopsy after prolonged course of high-dose tacrolimus. For 1 of the 3 patients, the post-LGI biopsy indicated new acute endothelial injury concerning for possible irradiation-induced kidney injury which correlated to a rise in serum creatinine after irradiation. All 3 patients maintained graft function through follow up of 4 months, 1 year, and 7 years.
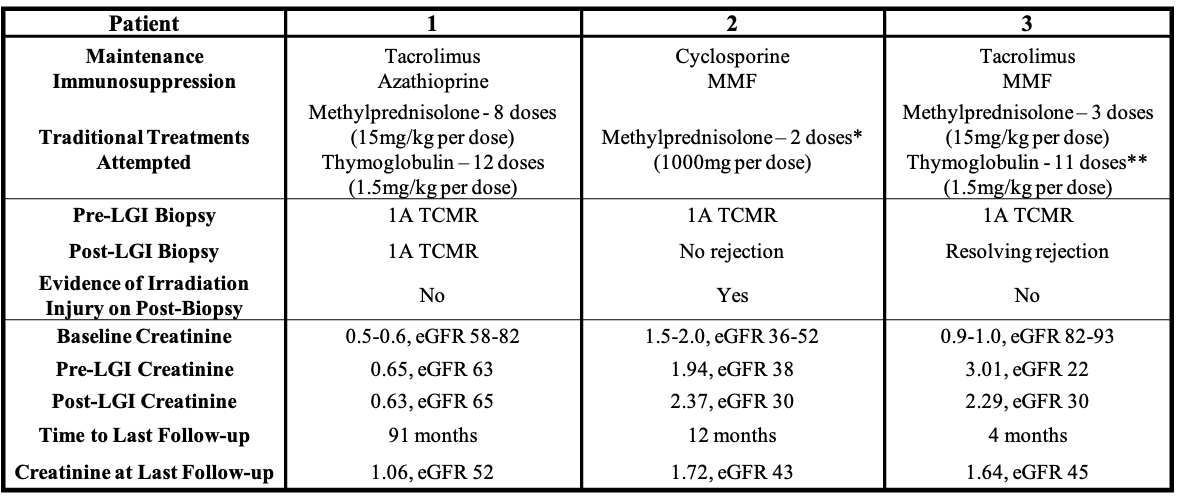
Conclusions: LGI may be a viable salvage therapy in pediatric patients experiencing acute TCMR refractory to traditional treatments or for those at risk of serious side effects. However, we are the first to report biopsy evidence of possible acute endothelial injury after LGI that may limit it's widespread use. Given our data, we suggest further studies to fully assess the efficacy and risk of this therapy in clinical practice.
[1] Halperin EC, Delmonico FL, Nelson PW, Shipley WU, Cosimi AB. The use of local allograft irradiation following renal transplantation. International Journal of Radiation Oncology, Biology and Physics. 1984;10(7):987-990. doi:10.1016/0360-3016(84)90168-8
[2] Jagetia R, Small W, Stuart FP, et al. Local graft irradiation after failure of modern immunosuppression in acute cellular and vascular graft rejection. International Journal of Radiation Oncology, Biology and Physics. 1996;36(4):907-911. doi:10.1016/s0360-3016(96)00340-9
[3] Noyes WR, Rodriguez R, Knechtle SJ, et al. Radiation therapy for renal transplant rejection refractory to pulse steroids and OKT3. International Journal of Radiation Oncology, Biology and Physics. 1996;34(5):1055-1059. doi:10.1016/0360-3016(95)02159-0
[4] Chen LM, Godinez J, Thisted RA, et al. New scoring system identifies kidney outcome with radiation therapy in acute renal allograft rejection. International Journal of Radiation Oncology, Biology and Physics. 2000;46(4):999-1003. doi:10.1016/s0360-3016(99)00474-5
[5] Nuyttens JJ, Harper J, Jenrette JM, Turrisi AT. Outcome of radiation therapy for renal transplant rejection refractory to chemical immunosuppression. Radiotherapy and Oncology. 2005;74(1):17-19. doi:10.1016/j.radonc.2004.08.011
[6] Wahl AO, Small W, Dixler I, et al. Radiotherapy for rejection of renal transplant allografts refractory to medical immunosuppression. American Journal of Clinical Oncology. 2006;29(6):551-554. doi:10.1097/01.coc.0000231452.47998.88
[7] Fallahzadeh MK, Khan S, B. Zibari G, Patil S, Singh N. Local graft irradiation for kidney allograft rejection: A case series and review of the literature. Nephro-Urology Monthly. 2014;6(3). doi:10.5812/numonthly.16262
