
Effect of Body Mass Index on Exercise Capacity following Pediatric Heart Transplantation
Alan Wang MD1, Kendra Ward MD1, Garett Griffith PhD, MPH1, Katheryn Gambetta MD1.
1Pediatric Cardiology, Ann and Robert H Lurie Children's Hospital, Chicago, IL, United States
Introduction: The prevalence of overweight and obese children in the United States has significantly increased in the past three decades. This trend negatively affects pediatric heart transplant (HT) recipients as prior studies have shown that obesity, dyslipidemia, and impaired exercise tolerance following HT increases the risk of cardiac allograft vasculopathy, graft loss, and post-transplant mortality. Cardiac rehabilitation programs following HT have been shown to significantly increase exercise capacity and are associated with decreased long-term mortality in adult studies. The association between body mass index (BMI) and performance on cardiopulmonary exercise testing (CPET) has not been studied for pediatric HT recipients. The aim of this study is to evaluate the effect of BMI on markers of exercise capacity of HT recipients and compare this effect with a healthy pediatric cohort.
Methods: A retrospective analysis of our institutional CPET data between 2004 – 2022 was performed. All patients exercised on a treadmill using the Bruce protocol. Patients were included in this study if they were between 6 – 21 years of age, had a history of HT (HT cohort) or no prior cardiac diagnosis (control cohort) at the time of CPET, and had a maximal effort test (respiratory exchange ratio ≥ 1.10). Patients were further stratified within these two cohorts as underweight, normal, overweight, and obese based on BMI percentiles. Males and females were analyzed separately. Two-way analyses of variance (ANOVA) were performed with diagnosis and BMI category as the independent variables. Exercise tests in which patients were pacemaker dependent were excluded from analysis.
Results: A total of 196 CPETs following HT and 1,782 CPETs of healthy patients were included in these analyses (Table 1).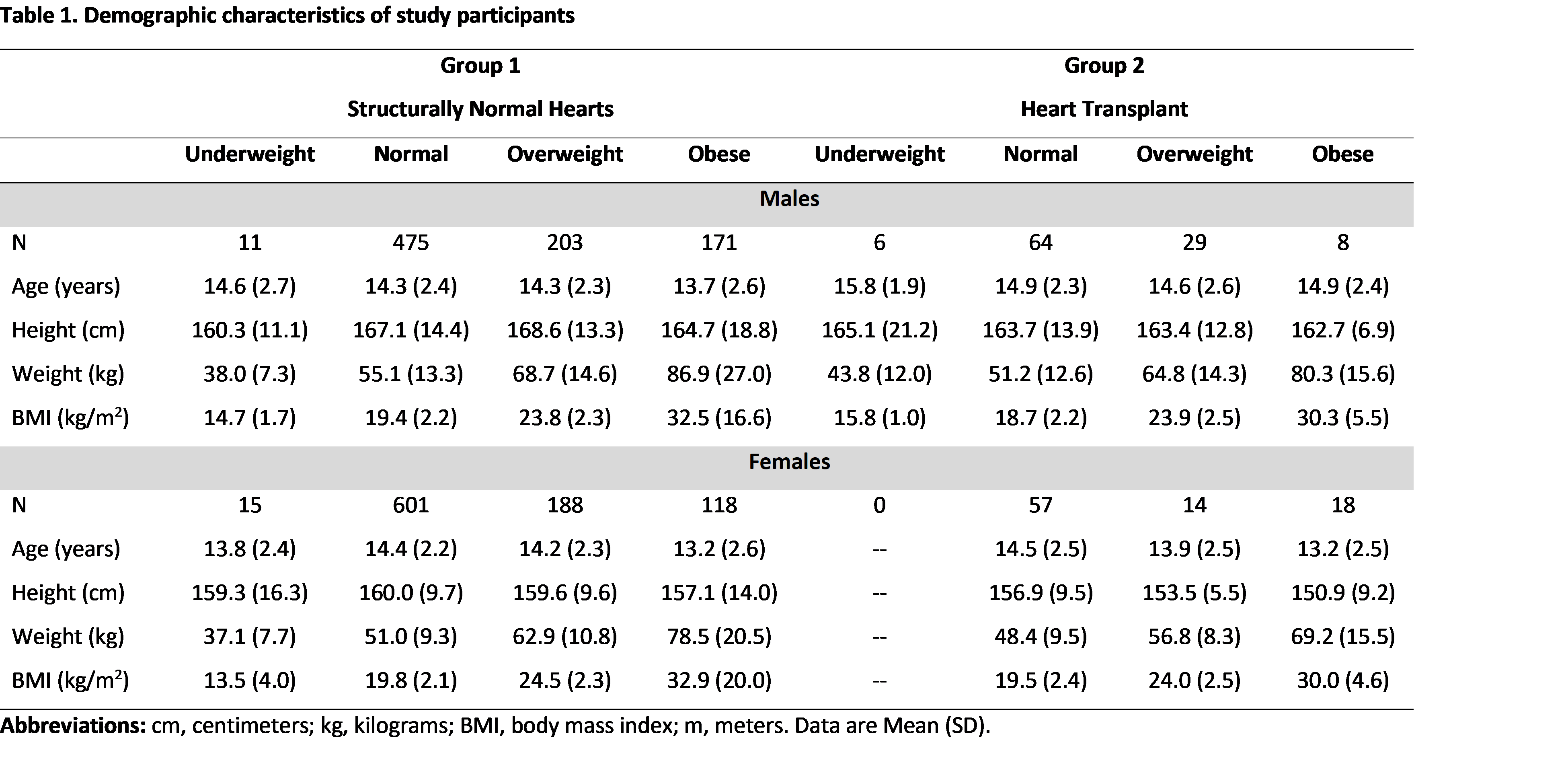 HT patients across all BMI percentiles had higher resting heart rates (HR, p<0.001) and lower maximal HRs (p<0.001), HR recovery at 1 minute (p<0.001), HR reserve (p<0.001), exercise duration (p<0.001), and peak aerobic capacity (VO2peak, p<0.001) when compared to a healthy cohort (Table 2).
HT patients across all BMI percentiles had higher resting heart rates (HR, p<0.001) and lower maximal HRs (p<0.001), HR recovery at 1 minute (p<0.001), HR reserve (p<0.001), exercise duration (p<0.001), and peak aerobic capacity (VO2peak, p<0.001) when compared to a healthy cohort (Table 2).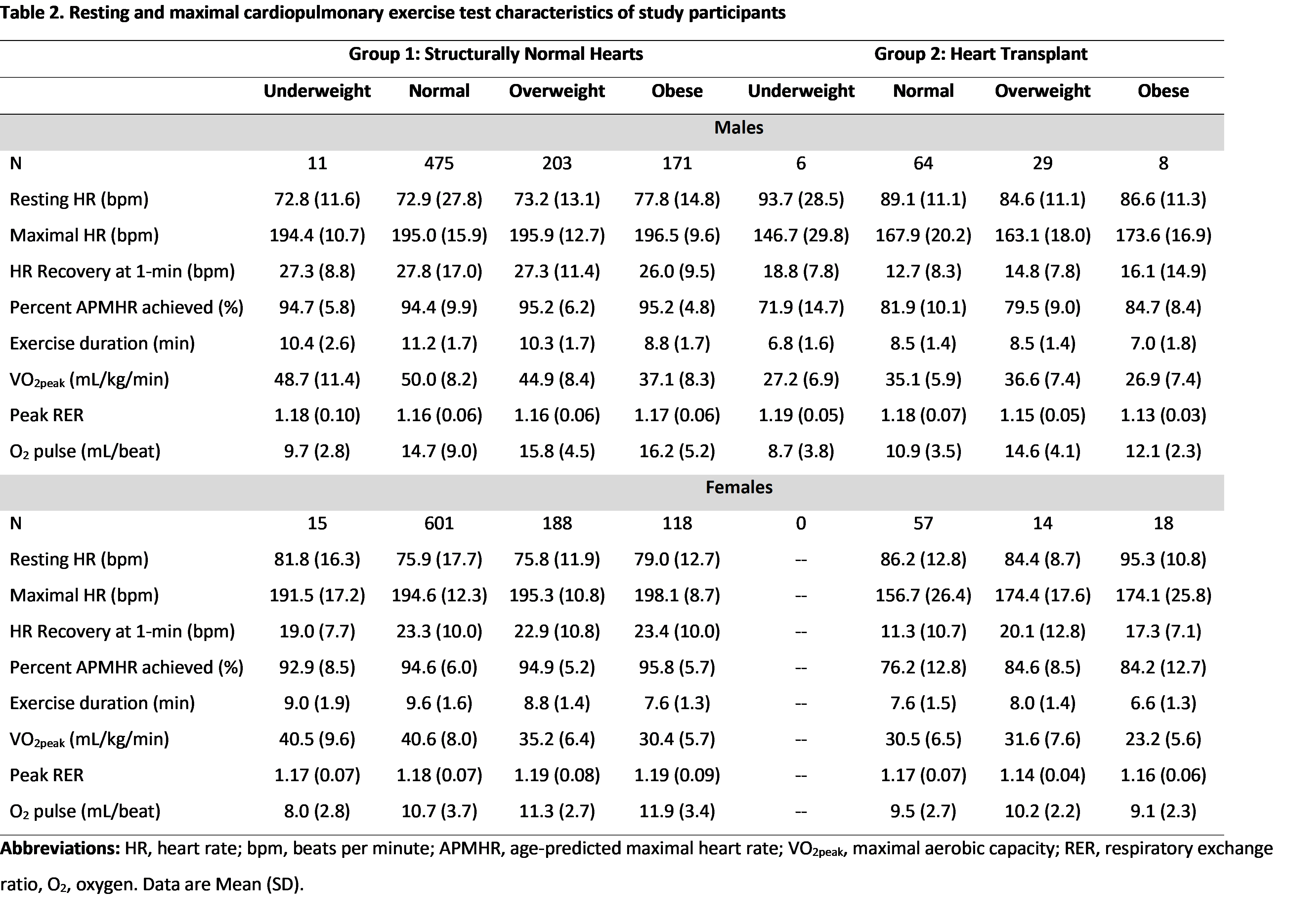 Both male and female HT patients in the normal and overweight BMI categories had significantly higher VO2peak (p<0.001) and exercise duration (p<0.001) when compared to obese patients. There were no CPETs of underweight females following HT and 6 CPETs of underweight males. Underweight males had reduced VO2peak (p=0.002) and exercise duration (p<0.001) when compared to normal weight males. This pattern was not present in our healthy population.
Both male and female HT patients in the normal and overweight BMI categories had significantly higher VO2peak (p<0.001) and exercise duration (p<0.001) when compared to obese patients. There were no CPETs of underweight females following HT and 6 CPETs of underweight males. Underweight males had reduced VO2peak (p=0.002) and exercise duration (p<0.001) when compared to normal weight males. This pattern was not present in our healthy population.
Conclusion: Obesity is strongly associated with lower VO2peak and exercise duration in both healthy and HT patients. Underweight males following HT have lower exercise capacity and may serve as a marker of fragility as this pattern is not seen in the healthy cohort. There were no significant differences in exercise capacity between HT patients in the normal and overweight categories. Patients with the best markers of exercise capacity following HT were those in the normal or overweight categories.
