BK viruria in pediatric heart transplant patients and its correlation with kidney function-A Single center retrospective study
Ruchi Gupta Mahajan1, Sarah Kizilbash1.
1Pediatrics, Division of Nephrology, University of Minnesota Masonic Children's Hospital, Minneapolis, MN, United States
Background: BK nephropathy is a significant cause of morbidity and mortality in kidney transplant recipients. Although BK infection has been reported after adult heart transplants, little is known about the prevalence and outcomes of BK viruria in pediatric heart transplant recipients.
Objective: To describe the characteristics and clinical course of BK viruria in pediatric heart transplant recipients
Methods: We reviewed all heart transplants performed in children (age < 18 years) between 1/2012 and 1/2022 to identify recipients with BK viruria. BK virus was detected in the urine using real-time quantitative BK Virus assay (reference < 1 copies/ml). We used the modified Schwartz equation to determine the estimated glomerular filtration rate (eGFR). Data are summarized as median with interquartile ranges (IQR) and proportions.
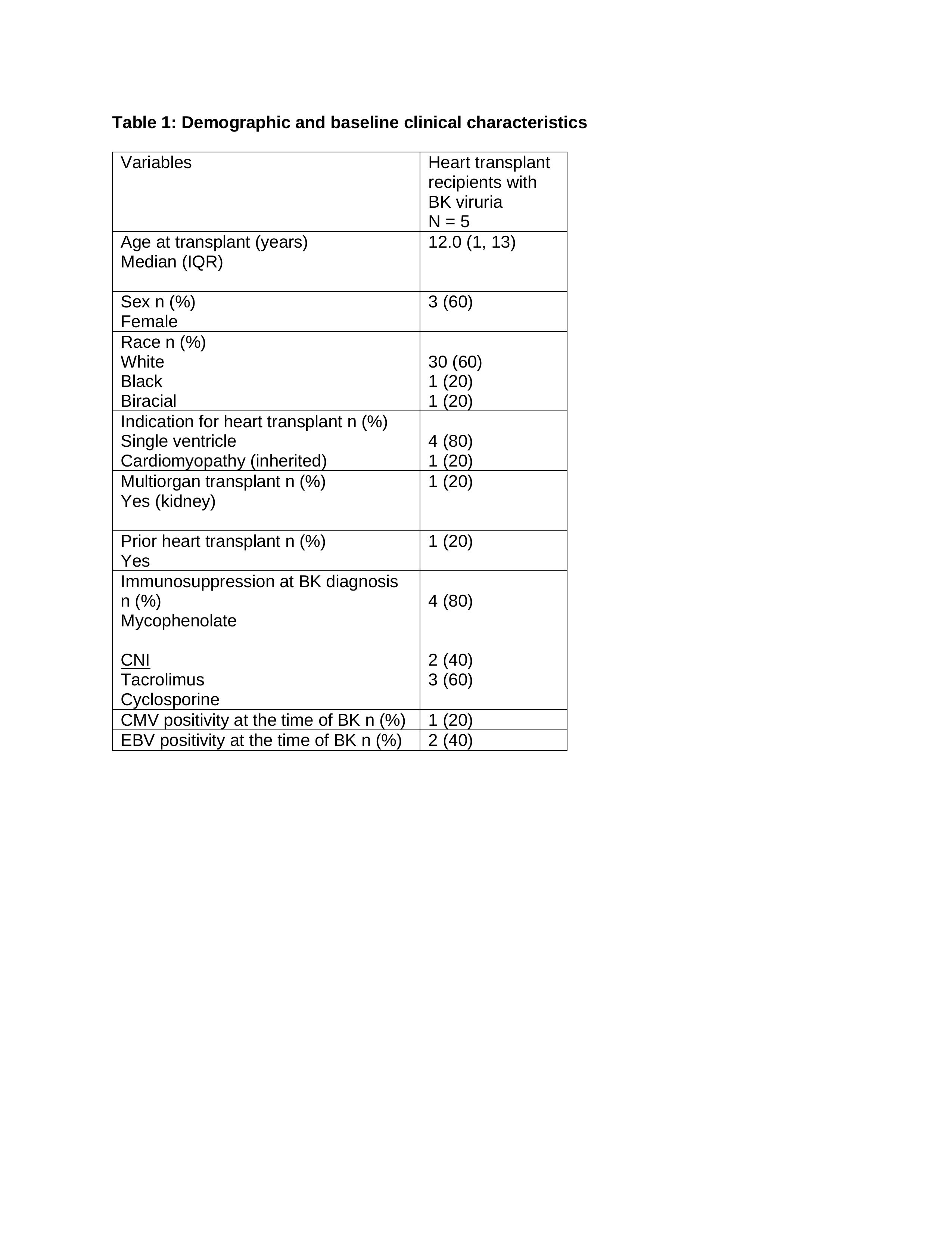
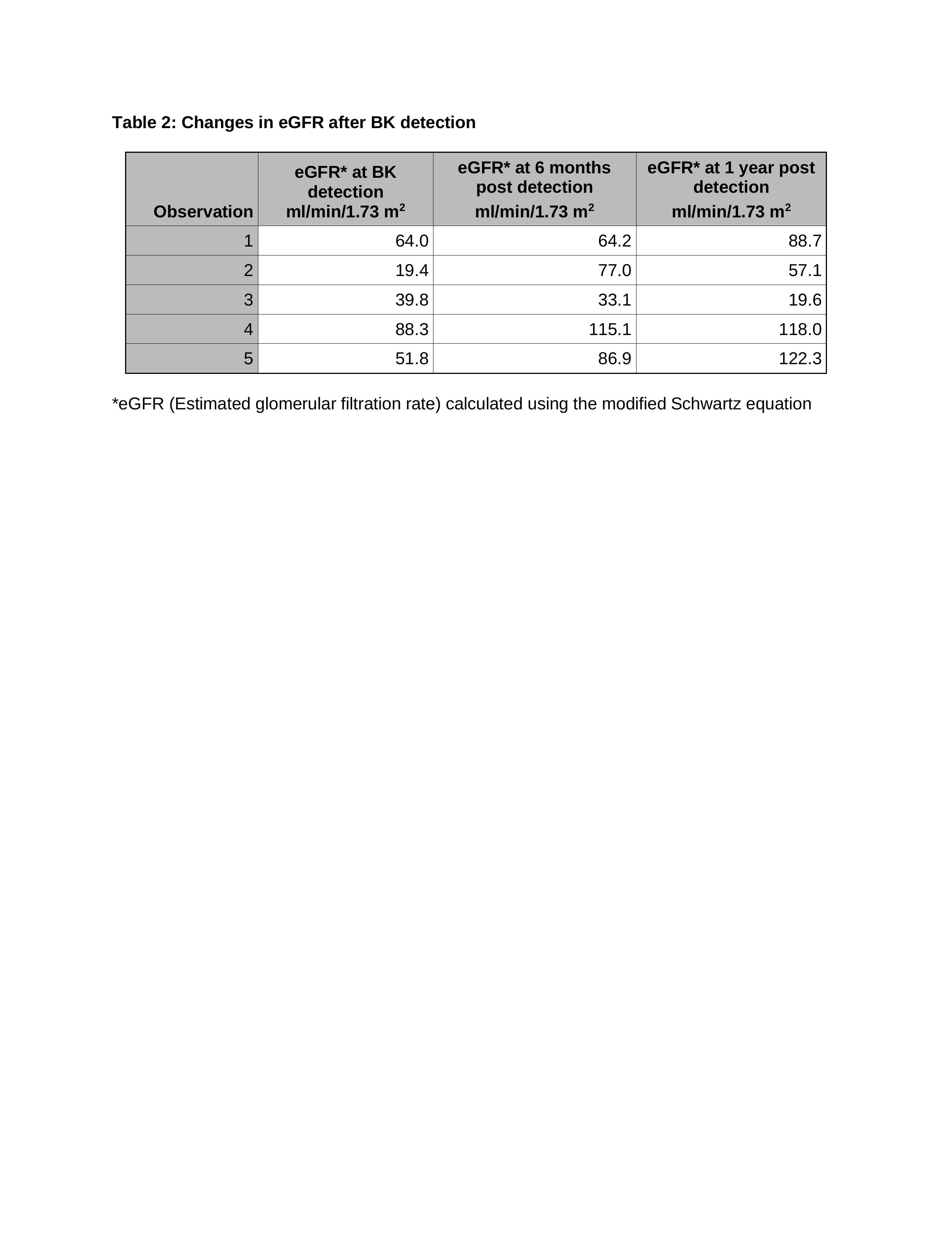
Results: BK viruria was detected in 4 pediatric heart transplant and 1 pediatric heart/kidney transplant recipient during the study period. The baseline and clinical characteristics of all recipients are presented in table 1. The median time from transplant to urinary BK detection was 28.1 months (17.3, 61.9). The median urinary BK titer was 1,915,268 copies/ml (IQR: 30,400, 13,126,409). No patient underwent a kidney biopsy. We observed eGFR of < 90 at the time of BK detection and then no further decline in eGFR after BK detection at 6 months and 1 years, except in the patient with combined heart/kidney transplant (table 2). Of the 5 patients, three received no intervention for BK viruria, 1 heart only recipient underwent mycophenolate reduction with 4 weeks of ciprofloxacin, and 1 heart only recipient underwent mycophenolate reduction for concomitant CMV and EBV DNAemia. The time to BK resolution was 144 days for the combined heart/kidney recipient. Of the 4 heart only recipients, 3 showed intermittent BK positivity over a follow-up ranging from 20 to 61 months, and one patient did not have BK rechecked after the initial test.
Conclusion: BK viruria may be seen in pediatric heart transplant recipients. We observed GFR< 90 at the time of BK detection and then no decline in eGFR after urinary BK detection at 6 months and 1 year except in a patient with combined kidney transplant. Additional studies are required to examine the prevalence, risk factors, and outcomes of BK infection in this population.
Lectures by Ruchi Gupta Mahajan
| When | Session | Talk Title | Room |
|---|---|---|---|
|
Sat-25 18:00 - 19:15 |
P6- Kidney Posters | Prevalence of nocturnal hypertension in pediatric kidney transplant patients using 2022 ABPM guidelines | Zilker 1-2 |
|
Sat-25 18:00 - 19:15 |
P5- Infectious Diseases Posters | BK viruria in pediatric heart transplant patients and its correlation with kidney function-A Single center retrospective study | Zilker 1-2 |