
The mode of kidney replacement therapy (KRT) influences the carotid intima-media thickness (IMT) in children and adolescence
Carl Grabitz1, Moritz Pohl2, Niema Memaran1, Daniela Thurn-Valsassina1, Bernhard MW Schmidt3, Karolis Azukaitis4, Anke Doyon5, Franz Schaefer5, Anette Melk1.
1Department of Pediatric Kidney, Liver and Metabolic Diseases, Hannover Medical School, Hannover, Germany; 2Institute of Medical Biometry, Heidelberg University Hospital, Heidelberg, Germany; 3Department of Nephrology and Hypertension, Hannover Medical School, Hannover, Germany; 4Clinic of Pediatrics, Vilnius University, Vilnius, Lithuania; 5Division of Pediatric Nephrology, University Children’s Hospital Heidelberg, Heidelberg, Germany
4C Study Group.
Children requiring kidney replacement therapy (KRT) have an increased mortality mainly driven by cardiovascular (CV) disease (1). Because CV events in pediatric populations are rare, non-invasive measurement of intima media thickness (IMT) can serve as a proven surrogate marker of atherosclerosis in children. The purpose of this investigation is to elucidate how different KRT modalities affect the CV burden in children with CKD.
Our study uses data from the international multicenter prospective 4C (Cardiovascular Comorbidity in Children with CKD) study (2). From a total of 704 children, we investigated a longitudinal cohort including 273 patients initiating KRT with yearly IMT measurements, a mean follow-up time of 3 years and a maximum of 8.5 years. KRT modalities were categorized as dialysis, preemptive KTx and late KTx (after initial dialysis). Patients lacking IMT measurements before or after start of KRT were excluded. We employ linear mixed regression modeling as well as spline regressions for visualization.
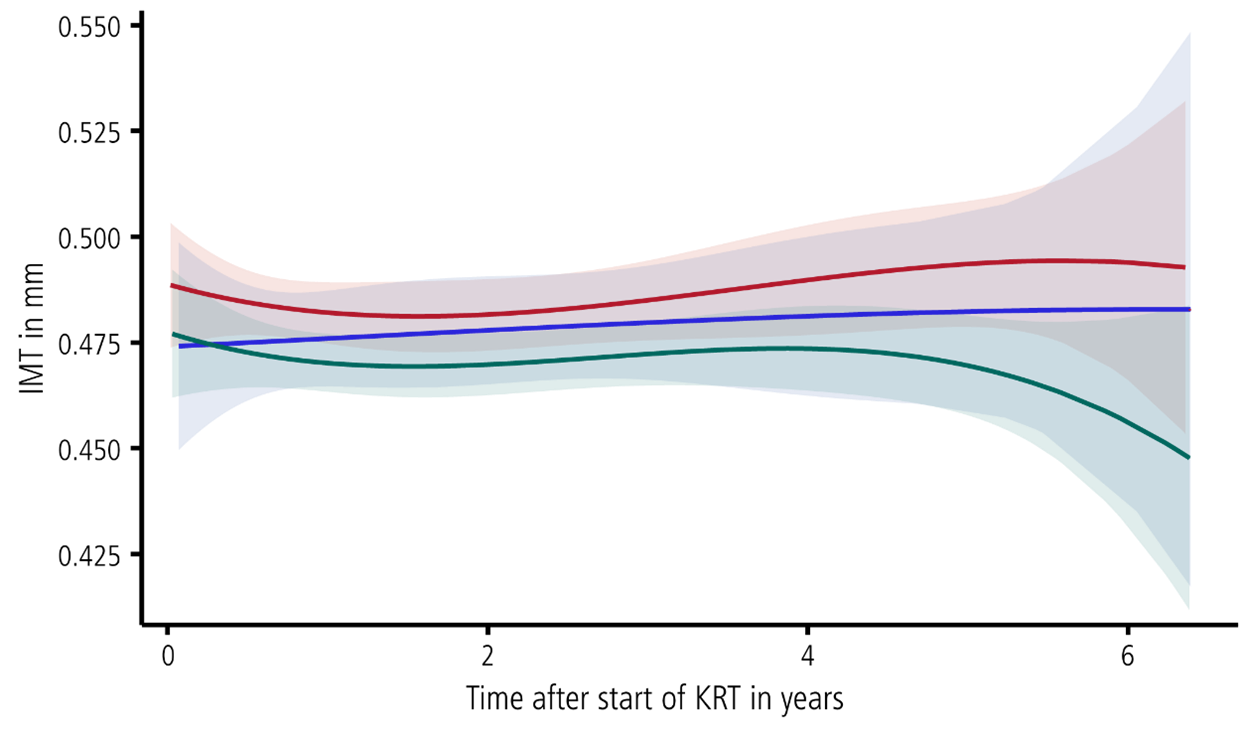
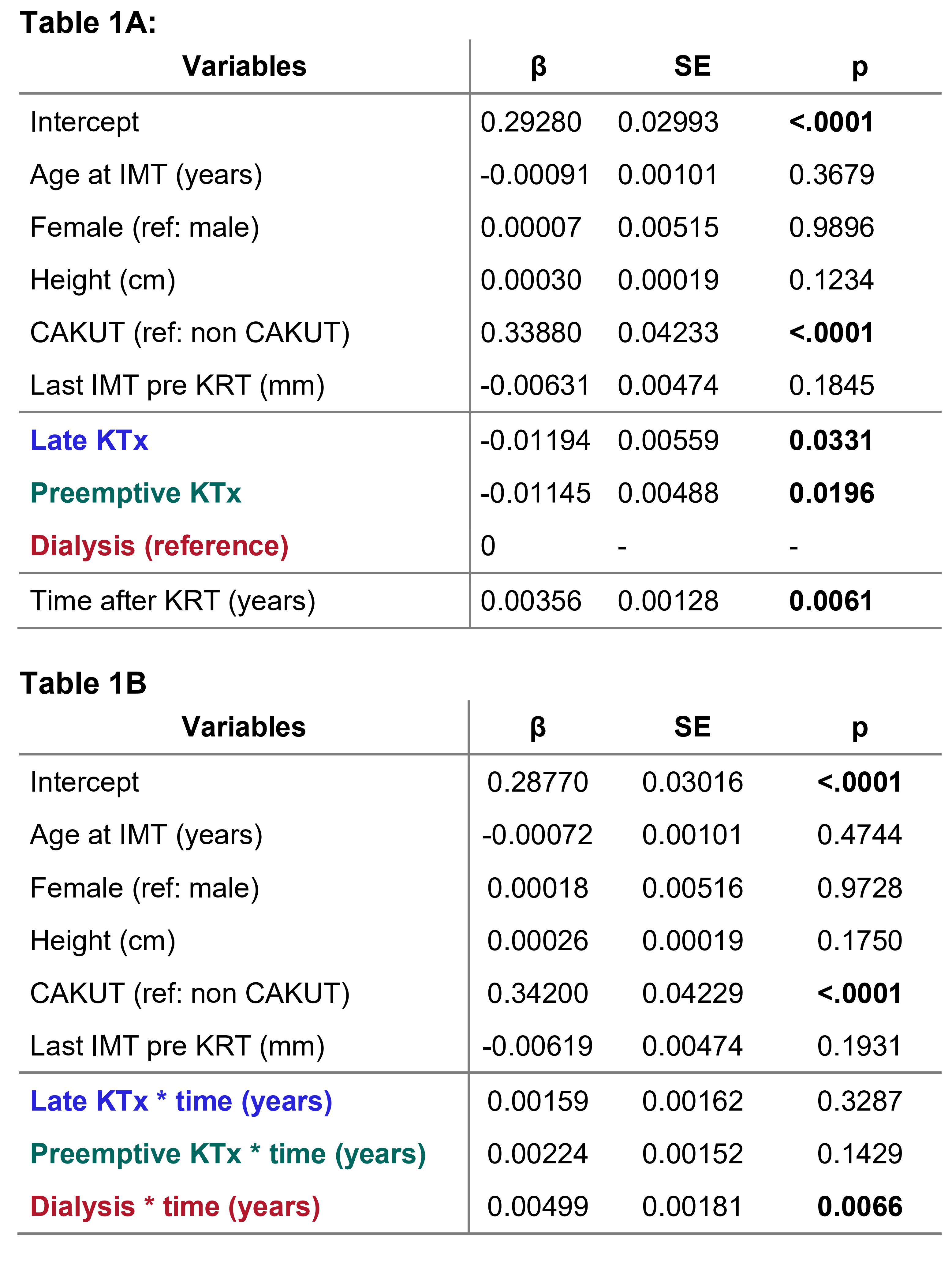
Patients’ characteristics where broadly similar between KRT modalities at their respective last visit during CKD. Spline regression indicated children after both preemptive and late KTx to have a lower overall level of IMT compared to patients on dialysis (Figure 1). This proved to be statistically significant in a mixed model corrected for age, height, sex underling disease and last IMT measurement before KRT start (Table 1A). A similar model including the interaction term of |KRT modality*time| revealed a significant progression of IMT over time during dialysis treatment only (β=0.00499mm/year, p=0.0066, Table 1B). The last IMT before respective KRT start was the most influential covariate in all mixed models (β from 0.257 to 0.518 with each p<0.001). High IMT under dialysis treatment was associated with higher systolic BP, lower BMI, lower serum albumin and lower bicarbonate. We did not observe a driving factor for IMT after KTx in our cohort.
In our longitudinal follow-up we found children receiving dialysis treatment to have higher IMT values that slowly increase over time highlighting the importance of blood pressure control, adequate calorie and protein intake as well as acid‑base homeostasis. In contrast, children after preemptive and late KTx demonstrated a stable course of IMT, which was not associated with any known risk factor, but with IMT before start of KRT.
[1] Bonthuis M, Vidal E, Bjerre A, et al. Ten-year trends in epidemiology and outcomes of pediatric kidney replacement therapy in Europe: data from the ESPN/ERA-EDTA Registry. Pediatr Nephrol. Aug 2021;36(8):2337-2348. doi:10.1007/s00467-021-04928-w
[2] Querfeld U, Anarat A, Bayazit AK, et al. The Cardiovascular Comorbidity in Children with Chronic Kidney Disease (4C) study: objectives, design, and methodology. Clinical journal of the American Society of Nephrology: CJASN. Sep 2010 2010;5(9):1642-1648. doi:10.2215/CJN.08791209
